



Ian Stewart, B.Sc.Phm., R.Ph.
The following is an example of a near miss that took place in a community pharmacy setting after transitioning from a hospital, and which was caught during the therapeutic check and resolved in collaboration with the prescriber. The analysis of the near miss is presented to highlight the learnings that can come from such cases along with possible quality improvements that a pharmacy team may implement into their practice to prevent future recurrence and patient harm.
Patients are at an increased risk of receiving an inappropriate drug therapy as they transition between healthcare providers and/or healthcare settings.[1]
Factors include lack of or poor verbal communication between healthcare providers and the patient prior to being discharged. Poor written communication (including the written prescription) and errors in converting parenteral therapy to oral therapy can also be contributing factors, as the case below highlights.
Pharmacists and pharmacy technicians must therefore be aware of the potential for a medication error when providing care to patients being discharged from hospital.
Case:
Rx:
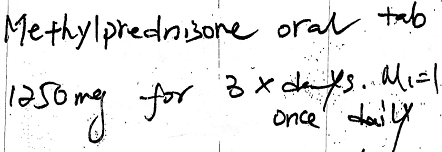

A hospitalized patient received 1000 mg methylprednisolone sodium succinate IV for the treatment of optic neuritis. Upon discharge, the patient was given the above written prescription. The patient took the prescription to his regular community pharmacy for processing.
The pharmacy assistant entered the prescription into the computer as methylprednisolone, though the prescriber wrote methylprednisone which does not exist. The pharmacist who checked the computer entry for accuracy failed to detect the discrepancy. However, during the therapeutic check, the pharmacist questioned the large unit dose of oral methylprednisolone.
An appropriate reference was consulted to identify an indication for such large oral unit dose of methylprednisolone. The pharmacist failed to find any indication for the oral administration of 1250 mg methylprednisolone. The prescriber (an ophthalmologist) was therefore contacted for confirmation of the dose of oral methylprednisolone and the indication for use.
It was determined that the prescriber wrote the prescription for methylprednisolone (misspelled) because the patient has received methylprednisolone sodium succinate IV while hospitalized. In addition, the prescriber acknowledged that they should have written the prescription for 1250 mg prednisone and not methylprednisolone.
Recommendations:
- Be aware of the potential for medication errors as patients transition from hospital to returning home.
- Whenever possible, gather information regarding the patient’s drug therapy while hospitalized and assess the appropriateness of the current drug therapy. The medication given in a hospital may be an alternative route/dose so consideration must be given to the drug, route and dose and understanding how it is being used.
- In addition to checking the computer entry for accuracy, the drug therapy must always be assessed for appropriateness. This is critical for both new and refill prescriptions. Factors to be considered include the patient parameters, medication history, indication for use, the dose, dosing interval and duration of therapy. It may be beneficial to complete the computer entry check, then complete the therapeutic check to ensure appropriate attention is given to both checks.
- Develop a process to ensure the indication for use is always collected (ideally before the prescription is processed) as it would be difficult to complete the therapeutic assessment without this key piece of information.
- Maintain easy access to therapeutic references to ensure the drug, dose, dosage form, dosing interval and duration of therapy is appropriate based on the indication for use and patient’s parameters.
- Be aware of the potential for confirmation bias as there are many look alike drug names.
- Be aware of the potential for hesitancy in contacting specialists to discuss the appropriateness of any drug therapy. Do not assume that the specialist has additional information that you do not have. Make the connection to confirm.
Please continue to send reports of medication errors in confidence to Ian Stewart at: ian.stewart2@rogers.com . Sharing your experience can prevent similar occurrences at other practice sites.
Please ensure that all identifying information (e.g. patient name, pharmacy name, healthcare provider name, etc.) are removed before submitting.
- Anonymously record all medication incidents and near misses via the AIMS medication event reporting platform.
- Document appropriate details of medication incidents and near misses in a timely manner to support accuracy.
- Analyze the incident in a timely manner for causal factors and commit to taking appropriate steps to minimize the likelihood of recurrence of the incident.
- Promptly communicate the appropriate details of a medication incident or near miss, including causal factors and actions taken as a result, to all staff.
Hospital to Home—Facilitating Medication Safety at Transitions. Institute for Medication Safety Canada: 2015. https://www.ismp-canada.org/transitions/ ↑