 Pharmacy Connection
Pharmacy Connection
Ian Stewart, B.Sc.Phm., R.Ph.
Though a larger number of prescribers are using computerized software to generate prescriptions, many prescribers continue to write prescriptions by hand, which increases the potential for misinterpretation.
To ensure the correct interpretation of the prescriber’s intent, the importance of completing a therapeutic patient assessment cannot be over-emphasized, as the following case highlights.
Case:
Rx:
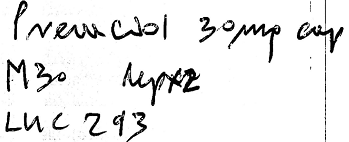
A seventy-five-year-old patient presented the above prescription to her local community pharmacy for processing. Upon entering the prescription into the pharmacy computer, the pharmacy assistant misinterpreted the prescription as the brand name drug “Pravachol” (pravastatin) instead of “Prevacid” (lansoprazole) as intended by the prescriber.
The pharmacist who checked the computer entry for accuracy failed to detect the input error. The pharmacist then proceeded to complete the therapeutic check but failed to identify the entry error despite the numerous red flags present. These included:
- Pravachol (pravastatin) is not available in a 30mg dosage unit.
- Pravachol (pravastatin) is not available as a capsule.
- Pravachol (pravastatin) does not require a Limited Use code.
- The patient was taking atorvastatin at the same time.
- The pharmacy computer software indicated a therapeutic duplication due to the two statins.
As a result of missing these red flags, unfortunately a generic brand of Pravachol (pravastatin) was dispensed to the patient with the instructions to take three 10mg tablets once daily. The patient took the pravastatin for three days before contacting her physician for information about the new drug. Fortunately, the patient did not experience any side effects.
Possible Contributing Factors:
- The written prescription was not clear and legible.
- The pharmacist failed to assess all aspects of the prescription. If the pharmacist had identified the misaligned strength and dosage form (Pravachol is not available in 30mg or capsules), perhaps these important prescription clues could have helped the pharmacist identify the error.
- The patient’s medication profile was not accessed to identify previous and current drug therapy. If the medication history was accessed, the pharmacist would have noted that the patient had taken the generic form of Prevacid (lansoprazole) previously and was taking atorvastatin at the time.
- No patient counselling took place. There was a failure to recognize that the medication was new for the patient, and/or have reliable systems in place to ensure a pharmacist intervention and patient dialogue occurred prior to the release of any new medications. At the time of pick up, the patient may have assumed that she was receiving the generic version of Prevacid (lansoprazole) as previously, and therefore declined counselling.
Recommendations:
- To ensure the correct interpretation of written prescriptions, consider all aspects of the prescription including the drug, dosing unit, therapeutic dose, dosing interval, duration of therapy, indication for use etc.
- When processing both new and refill prescriptions, always review the patient’s profile including medication history to identify potential errors including therapeutic duplication, discontinued therapy, drug interactions, contraindications, etc. Assess the patient holistically, considering characteristics such as age and medical conditions.
- All drug therapies must be assessed for appropriateness before the medication is provided to the patient.
- When processing prescriptions, develop a system to gather relevant information from the patient, including the indication for use. It would be impossible to assess the appropriateness of any new drug therapy without knowing the purpose of the medication. Use open ended questions when gathering information from the patient, such as “what did the doctor tell you your medication is for?”
- Develop a system to ensure counselling takes place with every new prescription as this is usually the last opportunity to identify misinterpretation and other medication errors.
- If the patient is unable or unwilling to wait for counselling, consider a follow-up phone call. This is especially important if the indication for use has not been confirmed and hence the therapeutic assessment has not been completed.
Please continue to send reports of medication errors in confidence to Ian Stewart at ian.stewart2@rogers.com. Sharing your experience can prevent similar occurrences at other practice sites.
- Anonymously record all medication incidents and near misses via the AIMS medication event reporting platform.
- Document appropriate details of medication incidents and near misses in a timely manner to support accuracy.
- Analyze the incident in a timely manner for causal factors and commit to taking appropriate steps to minimize the likelihood of recurrence of the incident.
- Promptly communicate the appropriate details of a medication incident or near miss, including causal factors and actions taken as a result, to all staff.










